With the suspension of Cincinnati Reds pitcher Edinson Volquez for performance enhancing drug use and a swirl of rumors that the agent involved was clomiphene (also known as Clomid,) I thought it timely to write about how clomiphene works and how it’s used. From what I read on the internets, there is an enormous amount of misinformation floating around out there.
To understand how clomiphene works, you need to know how the pituitary controls the making of testosterone in the testis. Testosterone is made by Leydig cells in the testis, which I explained in my last post. The pituitary releases a hormone called luteinizing hormone (“LH”) that stimulates the Leydig cells to make testosterone. Testosterone is converted to the female hormone estrogen, (which I also explained in my last post,) and estrogen tells the pituitary to stop making more LH. This kind of negative feedback system is common when it comes to how hormones work. It’s just like a thermostat and heater. As the room gets warmer, the thermostat sends less electricity to the heater. When the room gets colder, the thermostat sends more electricity to the heater.
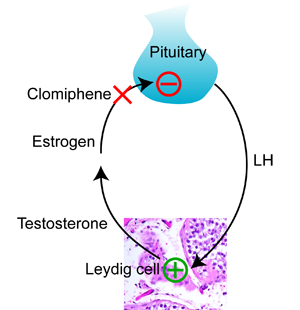
Clomiphene works by blocking estrogen at the pituitary. The pituitary sees less estrogen, and makes more LH. More LH means that the Leydig cells in the testis make more testosterone.
As I explained in my last post, giving testosterone to a man does just the opposite. The pituitary thinks that the testis is making plenty of testosterone, and LH falls. As a result, the testis stops making testosterone, and the usually high levels of testosterone in the testis fall to the lower level in the blood.
So clomiphene is a way to increase testosterone in the blood and the testis at the same time. It preserves testis size and function while increasing blood testosterone.
Unfortunately, clomiphene is not FDA approved for use in the male. Like most of the medications that we use to treat male fertility, the pharmaceutical company that originally sought approval by the FDA did it for women. Clomiphene is now generic, and it’s unlikely that anyone will pony up the hundreds of millions of dollars necessary to get it approved for the male. That’s the bad news. The good news is that it means that this medication is fairly inexpensive, cheaper than most forms of prescription testosterone. Can a doctor prescribe clomiphene for a man? Yes. It’s “off label”, meaning that it’s not FDA approved for use in men.
As a medication, clomiphene is usually well tolerated by men. In my experience, most patients don’t feel anything as their testosterone rises. Those that do feel an increase in energy, sex drive, and muscle mass, especially if they work out. Very rarely I’ve had patients report that they feel too aggressive, or too angry. Very very rarely (twice in the last 20 years) I’ve had patients report visual changes. That’s worrisome, as the pituitary is near the optic nerve in the brain, and visual changes suggests that the pituitary may be changing in size. Because the skull is a closed space, it’s alarming if anything in the brain changes in size. In the last twenty years, I’ve also had two patients who had breast enlargement (called “gynecomastia”) while using clomiphene. Needless to say, for any of these problematic side effects, the clomiphene is discontinued.
So that’s the story with clomiphene. It can be used in the male, either for fertility or low testosterone levels. It’s an off label prescription drug. It works, and is usually well tolerated by men who take it.
Hi, maledoc. I understand that we can’t ask you questions regarding are personal health problems or any other specific persons health problems. With that said I ask the following questions with the understanding that my questions and your answers pertain to anyone and not myself or any other specific person.
In general, do you or would you consider treating patients who complain of symptoms that could be indicative of Low Testosterone such as low sex drive, hot flashes, loss of lean muscle, loss of energy and trouble sleeping after they have taken steroids or Pro Hormones and experienced testicular shrinkage with Clomid, that have a Total Testosterone level that is in the Low normal range at the time they experience such symptoms?
Also, do you think that how successful the outcome of treatment with Clomid as far as the drugs ability to restore such a patient’s LH, FSH function and testicular size back to normal (when I say normal I am referring to what these levels and Testicular size were before taking the Steroids or Pro Hormones) depends on when a patient who experiences such symptoms under the above mentioned circumstances starts to take the Clomid after discontinuing the Steroids or Pro Hormones. In other words do you think that the outcome would be the same for a patient who waits six months before taking the Clomid as a patient who takes the Clomid admittedly following the Steroids or Pro Hormones.
Lastly what is your opinion regarding using Toremifene and Nolvadex for the purpose of restoring a patient’s ability to produce Testosterone after taking Steroids or Pro Hormones? Do you think these drugs are just as effective, more effective or less effective as Clomid when used for this purpose? Do you think these drugs have less or more side effects when comparing them to Clomid? Have you ever recommended to a patient to take a combination of anyone of these drugs at the same time for this purpose?
Hi Robert, so much goes into sex drive: sometimes it responds to changing testosterone, sometimes not. As for consequences of testosterone and testosterone-like medications, it depends on the man and how long he was taking them, with the longer the time, the higher the chance of irreversible changes. I’d recommend management by a qualified physician.
Ok, thanks.
And as far as attempting to treat a problem like this with Clomid? To reverse suppression that is caused by taking Testosterone? Is this something that you or other doctors attempt to do?
I answered that in a reply to a comment May 9th 🙂
Hi! From what I can tell from the packet insert of Clomid and a few other sources, the common dosage for women with infertility is 50 mg/day. Is the dosage for men (with low LH/FSH), as a rule, about the same or would it be higher/lower because men have different anatomies?
Hi Anton, if you scroll up a few comments, you’ll see that I’ve answered this a couple of times in a whole post for doctors on how I use clomiphene in the Doctor’s Corner.
Thanks, I had missed that there were older comments available.
Hi,
In one of your prior responses, you provided the following information:
“In some instances, the estradiol will increase, but as long as the ratio of total testosterone to estradiol is greater than ten-to-one, that shouldn’t be a problem”
I am curious as to how you go about determining what the Total Testosterone to Estradiol ratio is when you are interpreting a male patient’s blood work. (I am assuming it’s a simple math equation once you have a Total Testosterone and Estradoil reading)
I use the approach described by Schlegel in Aromatase inhibitors for male infertility. J Urol. 2002 Feb;167(2 Pt 1):624-9. The ratio is determined by dividing total testosterone in ng/dL by estradiol in pg/mL.
I ask this question with the understanding that my question and your answer do not pertain to me or any other specific person and is simple just for general knowledge
If you were seeing a patient in their mid twenties who’s LH was at 4 IU/L, FSH was at 3 IU/L and his Total Testosterone was at 366 NG/DL who recently was taking Testosterone for the purpose of putting on muscle and size at the GYM and that once he experienced testicular shrinkage he decided to stop taking it and now sense stopping the Testosterone supplementation continued to feel weak, tired and hot flash sensations in his head, would you try treating him with Clomid?
Robert, I really think you (or that patient) needs to see a doctor familiar with male endocrine issues and treatments.
LOL. Im off to Endo number 5 next week.
but I still got more info from your Blog than I did from the four useless Endo’s I have seen so far, so thanks anyways
What would you consider to be a high FSH/LH? IF FSH is in the 4-5 mIU/ml range, and LH in the 5-6 mIU/ml – with low total testosterone below 200 – would this mean the patient might be a good candidate for temporary Clomid treatment?
Also – have you encountered a relationship between hypothyroidism in men and hypogonadism? Can one cause the other?
I’ve noticed that many of the hypogonadism and hypothyroidism symptoms seem to overlap. Are there any prime indicators to tell one from the other?
Thanks so much.
Great questions all. Keep in mind that LH and FSH are not coupled in the male as they are in the female. As a marker of sperm production in the testis, we’ve argued that 7.6 IU/L is a good threshold for FSH. Any time that the LH is low compared to testosterone production indicates low pituitary function that may respond to clomiphene or other stimulatory medications. There is an association between hypothyroidism and low testosterone, and those patients may respond to thyroid treatments, but it’s infrequently encountered. You’re right about the overlap in symptoms, which makes identifying those few hypothyroid patients difficult.
Great job doc informing people with facts rather than all the conflicting bs you read on the internet.
Now the question:
What is your experience with long term usage of Clomid in men ? Any side effects that might be harmful ?
Thanks, Patrick! I outline my own experience as a physician observing side effects in the second to the last paragraph of that post. Unfortunately, as clomiphene is off patent, it’s unlikely that we’ll get good long term data on its use.
Hi doc…Can clomid be used to treat gynecomastia as in breast tissue there are estrogen receptors and if they are blocked by clomid it can lead to shrinkage of breast tissue. .What are your views about it?And can there be rebound gynecomastia once the medication is stopped as there are raised estradiol levels in the blood due to clomid intake(due to increasd testosterone conversion to estrogen by aromatase)..
I’ve not known clomiphene to be used to treat gynecomastia, and it doesn’t make sense to me biologically that it would help. On occasion, if estradiol increases sufficiently, clomiphene use may be associated with gynecomastia.
Thanks
Hi MaleDoc: I apologize if this has been asked/answered many times, but my impression is that the majority of your patients don’t experience the the desired benefits, or magnitude of those benefits, generally attributed to the use of testosterone (e.g., cypionate) including increased lean muscle mass, strength, vigor, positive outlook, etc. Is my impression at all accurate? Thanks for graciously answering so many questions!
Hi Brad, in my experience, it’s the level of testosterone in the blood that counts, not the way that it gets there.
My initial post might not have been very clear. I was asking, based on your opening statement that “In my experience, most patients don’t feel anything as their testosterone rises. Those that do feel an increase in energy, sex drive, and muscle mass, especially if they work out,” roughly what % of patients have experienced the foregoing results. Thanks again Doctor.
Hi Brad, most of the patients that I treat are interested in fertility, and don’t have other symptoms of low testosterone such as decreased sex drive and energy. Most don’t feel differently as their testosterone increases.
Dr, I just wanted to thank you for the information. I finally understand what my endocrinologist is up to. I’m starting second week of the medication (no results). This week I was told to double current dose of half a tablet. We don’t have a diagnosis yet but very low T, zero LH, low end of FSH and small “common” tumor found on m.r.i and in my early 30’s. If this new dose isnt effective do patients ever take clomid and testosterone together?Thanks for reading.
Hi Ryan, I’m sorry, but I can’t answer personal questions about your own health. Please read the FAQ.
Hi, in your post regarding how you prescribe Clomid in men you mentioned that “in some instances, the estradiol will increase, but as long as the ratio of total testosterone to estradiol is greater than ten-to-one, that shouldn’t be a problem.”
With that said I understand that you recommend that while a man takes Clomid he should have Blood work done to make sure the ratio stays greater than ten to one.
My question is, is there any drug available that you have ever had a man take while the takes Clomid to prevent or decrease Estrogen levels all together.
I notice that there is a lot of information floating around on the internet that suggests that there are such drugs that have the capability to act as “Estrogen Blockers.” I feel as if this information comes from people’s misinformed understanding on how a drug like Clomid works by Blocking Estrogen at the Pituitary and not prevention Estrogen from just being there in the first place. Am I correct on this?
Robert, you inspired me to post about aromatase inhibitors. Hop on over to More Pills and Testosterone, and thanks!
Thank you so much for all this info
Hi Doc,
I have been on clomid for the past five months due to having secondary hypogonadism. I do notice that I have more energy than before however I still feel that I have a lack of interest and I am unmotivated to do things. I tried the androderm patch before clomid and it worked well for the first few months as I can say I was feeling somewhat normal. I had to stop the patch because it eventually gave me a bad rash on and around the placement points. One of the other side effects of the patch and also the gel is that a depression came over me like none other. I have not had my testosterone checked since I started taking clomid however it has been checked for all the routine exams. My red blood cell count and hematocrit levels are high which a dermatologist has mentioned this may be the cause for my skin itching all over. They said it was PV or Polycythemia Vera. I was wondering if this might be a side effect of taking Clomid. I am considering stopping the clomid to see if my red blood count levels go back to normal. Instead of clomid I have also been considering trying testopel. The issue there is that I am concerned with my testicles shrinking and me losing the ability to have children someday. Any thoughts or comments?
Thanks
Brian
I’m sorry, Brian, but I can’t answer personal questions about your own health. Please read the FAQ.
Hello doctor,
A few months ago I found out that I have low sperm count. I gave 3 samples 3-4 weeks apart from each other, and the results were 2 million, 9 million and 2 million. I have been prescribed 50mg Clomid which I have been using every day for the last 2 months. Next month I will be giving another sample for analysis. How likely is it, that in a month, my test results will be higher, more than 20 million ? In case that Clomid doesn’t work, are there any other fertility drugs that I can use to increase my sperm count? Thank you.
Sorry, but I can’t answer personal questions about your own health. Please read the FAQ.
SUCCESS! He started clomid and I got pregnant in a month and a half. I’m 7 weeks yesterday!
doc,
When treating a patient with low testosterone with Clomid,
1,how long do you have him take clomid ? and
2. how do you know when it is time to discontinue treatment ?
cheers
Hi Andy, it depends on the patient and what’s needed from therapy.
A testosterone replacement specialist at renewman.com advised me that Clomid by itself can boost the body’s own ability to generate testosterone up to the optimal levels for a man age 30 or 35. But for someone age 50, this specialist said Clomid is not strong enough to get free testosterone in the 20 – 30 range. On the other hand, if a man relies solely on testosterone gels or creams, then his body’s hormone system will atrophy: shrinkage not only of the testicles but also the pituitary. Given these two facts (1) Clomid by itself will not produce optimal testosterone levels for men over, say, age 45, and (2) testosterone supplements will cause the body’s natural hormone system to atrophy, then the remaining solution is to use a hybrid Clomid + testosterone supplement therapy. Do you agree? Finally, for long term (30 or 40 years), it makes more sense to combine Clomid with testosterone than hCG with testosterone, because hCG will only stimulate the testes and leave the hypothalamus – pituitary axis atrophied.
Hi Michael, I’d say that someone needs to see, in person, a physician with a background and experience in treating men with low testosterone. Those “facts” are certainly not what I’ve observed over the years, nor do they make biological sense.
Are you familiar with Clomifene Citrate? Is this the same thing as Clomiphene citrate but just the generic version?
It’s the same, just an alternate spelling.
Hi Doc
You mention in the introduction to this blog that clomiphene has the effect of increasing the amount of Leutinizing hormone released by the pituitary. Therefore, would you only consider clomiphene treatment if LH was low? If so, what would you consider low?
Thanks
Colin
Hi Colin, I answer that in the Doctor’s Corner post.
Sorry I should have read that. You say 25 is too high…what would you say is low enough? Thanks
Below that number, if treatment were indicated, I would recommend it.
Thanks
Have you found Clomid to have negative reactions with anti-anxiety medicine(ie Wellbutrin, Trazadone, etc?
Does Zinc levels play a role in testosterone levels? If so, how?
Thank You…
Hi Chris, sorry that it took a while to get to your post: I’ve been on vacation 🙂 I haven’t observed clomiphene to specifically interact negatively with typical anti-depressant medications. Some of these medications suppress testosterone, and I’ve treated men with clomiphene to restore their testosterone levels. As you can imagine, depression itself can change sex drive, and it often requires working closely with both the patient and his therapist to have the best shot at improving the problem. I don’t believe that Zinc plays a great role in testosterone production.
Thank you
If Clomid can raise LH & FSH, what happens if these fall outside the normal testing range(ie FSH 20 or higher).
The question above refers to FSH & LH raising due to the clomid ie FSH 20.
Hi Chris, as clomiphene works by increasing LH, an increase in LH is a sign that it’s working in the way that it is intended. FSH and LH are uncoupled in the male, unlike in the female. Consequently, FSH rises variably in men taking clomiphene. If it increases, that’s likely a sign that the environment for sperm production is improving. This can be confusing, as a high FSH without treatment means that the sperm factory is not working well.
Thanks – you do a great service.. Nice that you do this for everyone.
Hi Maledoc, extremely informative blog! A quick scnerario:
24th Feb 11: Prolactin: 8 ug/L, Testosterone: 10.1 nmol/L, Estradial: 51 pmol/L, LH: 3.44 IU/L, FSH: 3 IU/L, SHBG: 19.8nmol/L
after 2 months of Tribulus:
Testosterone: 8.4 nmol/L
SHBG: 12.2 nmol/L
Followed by 2 months course of herbal supplement; which are supposedly the natural T boosters:
Tribulus Terrestris: standardized for 80% steroidal saponins as well as 30% protodioscin.
Avena Sativa: standardized for 15% steroidal avenacosides A & B
Eurycoma Longifolia (LongJack): standardized for 40% Glyco Saponins and 30% Polysacharides.
After this course, I am now planning to take the above combination with 50mg of Clomid for 3 months and repeat my T and SHBG levels.
In short, I am trying to increase my T levels.
My only concern is do you think this short course of clomid is likely to aggravate my already existing “mild” gynaecomastia???
Thank you so much for your kind reply!!
Manish from Singapore
Thanks, Manish! Unfortunately, I can’t answer personal questions about your own health. Please read the FAQ.
Nice resource you have here.
2 questions:
1) how long is clomid therapy for men typically precribed for?
2) Is a Urologist or Endocrinologist bettter equipped to handle secondary hypogandism?
thanks
Thanks, Patrick! For the first question: it depends on why the clomiphene is being prescribed. For the second, I know great urologists and endocrinologists that are well equipped to assess secondary hypogonadism and treat it. It’s one of those overlap areas in medicine where different specialists can treat the same problem well. However, ask the urologist or endocrinologist how often they encounter it, and you’ll get an idea of their experience.
I meant if it is being prescribed to treat secondary hypogandism. For instance, I know it sometimes used as a first course to try and “restart” a man’s own testosterone production, before resorting to TRT.
But at what point do you decide clomid isn’t going work and resort to other alternatives if the patient isn’t responding?
In other words, how long is it considered safe for a man to stay on clomid continuosly? (e.g. 6 months, a year?)
Thank you for your time.
Hi Patrick, as clomiphene isn’t FDA approved for use in the male, we unfortunately don’t have the typical safety data, and as for many drugs, we don’t have long-term safety data. As for deciding when clomiphene isn’t working, that is on an individual basis as different men respond differently to the drug.
Good morning, have not seen such a useful forum, this topic is rescued me. Thanks to the author))
Thanks! Feel free to link to it 😉
Quite a lot of time spent to find this information in the network. Not yet stumbled on this topic.
Hi Doctor,
Thanks for answering all of these questions.
My question is with regard to starting Clomid with a concern over the potential of an undiagnosed adrenal problem. For example, if someone had a sudden drop in testosterone production, as well as thyroid function, while simultaneously developing an inexplicable and extreme overreaction to an unexpected stress event…could Clomid exacerbate this adrenal problem? I was reading the drug’s warnings, and it stated not to begin taking it if a person has [among other things] “uncontrolled thyroid or adrenal problems”.
Thanks very much.
I’m sorry, but this really sounds like a personal question about your own health. Please read the FAQ. You really need to see a doctor in person to answer your questions about your condition.
Do men taking clomid experience increased emotional feelings? I seem to have read that men sometimes get very weepy and can cry for no reason? Can clomid cause feelings of anxiety or worry?
If clomid is given to a man to increase T levels, how long is it given? Once stopped, will the T levels fall or will they remain the same?
Thanks for your information.
Patients haven’t reported that to me, but all sorts of side effects can happen with any medication. Read the comments above and my other posts: I’ve written about your second question a bit.
Hello Maledoc, first I’d like to say thank you for taking the time to write this blog. It has been incredibly valuable to me. Secondly, my husband has an upcoming appointment with you and we are wondering if you recommend any specific test results that we should have in hand for the appointment? He already has the semen analysis but would like to know if there are any blood tests that would be beneficial? I do understand if this is not a suitable forum for this information.
Thanks for your time.
Good to hear! I look forward to seeing him, and I’ll wait until I have an opportunity to meet with him, examine him, and review the semen analysis before recommending testing.
Hey. Does clomid help sperm motility? Does it help them to swim if not many are? I am just unclear of what fertility drugs can help get sperm swimming if any.
Thank you
Hi Dave, It may if the sperm motility is secondary to low testosterone in the testis. If it’s another cause, then probably not. Unfortunately we don’t have a way of accurately assessing the first with laboratory testing, and so a common strategy is to treat if the blood testosterone is low, and see if motility improves.
Have you heard of clomid lower sperm counts instead of raising them?
My husband has low sperm count (4-6 million total). There is no cause for his low counts so his urologist prescribed clomid 50mg daily for 3 months and then do a SA.
Before starting the clomid fsh, lh, and testosterone were tested and they were all normal, though testosterone was in the 300 range (my husband had just turned 34 at the time). Anyways 3 months after starting the clomid his count dropped to 20 thousand total. He never had bloodwork done except for the one time before starting the clomid. I blame the huge drop in his count on the clomid and wonder why and if it would go back up. Our urologist dropped us after this and just sent us to a RE ivf+icsi. I am wondering if it is worth it to try and find another urologist and get to the bottom of the cause for dh’s count issues or just give up on it. We have done 2 ivfs and have one child and I really would like to have one more but not do anymore ivfs since I am not a very good stimmer.
I’m sorry, CP, but I can’t answer personal questions about your husband’s personal health. Please read the FAQ.
hello doctor pls i just came across this forum and i decided to ask few questions about fertility.Am 37 yrs old and my husband is 52yrs old and we have been trying to have a baby for 5yrs now without no luck, so i have done all test which shows am vey ok, my period comes regularly and my man has 2kids before as well.He smokes and drink too and i dont know if clomid will help with his sperm, becaus i have been taking clomid for3monthes now, so pls advice me on what to do cos am confused,alot of fertility drugs on the internet, which i dont know what is best for us,thans as i await ur reply.
I’m sorry, Joy, but I can’t answer personal questions about your husband. Please read the FAQ.
Hi maledoc,
Great page with lots of info. My question is since medications such as HCG work by mimicking LH do they thus have no chance to correct any issues once treatment is stopped? Can Clomid be used as a way to try to jumpstart the pituitary to produce testosterone on its own, or is typically looked at as a long term treatment?
Thanks for your input
Thanks, Jake. I’ve been asked that question a number of times in various ways, so I wrote an FAQ about it.
Hi Doc
You mentioned before that when LH is below 25 it may be appropriate to use Clomid. In the UK the range is 3 – 12 for LH. Presumably there is a different unit being used. Do you know what the equivalent of 25 would be using the UK measurement?
Many thanks
Colin
Hi Colin, they’re both the same, international inits per liter (IU/L). 3-12 is the “normal” range, a statistical assessment. 25 is a high upper threshold.
Hcg 2 to 3 times a week then FSH added for a total of 3 weeks is the standard of practise for treating secondary hypogondism in males. In scondary hypogonadism which only accounts for 2% of the cases of male infertility, both LH and FSH are low, hence hormonal therapy is indicated. Keep in mind that hormonal therapy is not indicated in primary hypogonadism (40%) where TST is low, but FSH is ok. Hence my question, why do we use clomid instead of the standard practise? Esp since clomid would only increase LH and TST and little or no effect on FSH. Clomid is actually supposed to be used only for 5 days in women per month for a total of 6 cycles, but i just encountered a guy that has been on clomid for 7 months. I understand that hcg (Novarel, pregnyl and hmg (menopour) are both IM while FSH(gonad-F) is Sub.Q and that none of them comes as a tablet, so it might make sense to achieve increased LH using clomid, but then using it for 7 months? Is there anything am missing Dearest Author.
By the way, I want to thank you for this write up. It is superb. You know you stuff, my friend.
Thanks, PharmD. Treatment with clomiphene is at present standard practice for men with a responsive but insufficient pituitary. Women cycle but me don’t, which is why stimulatory medications are given in continuous fashion in the male.
hello doc
if testosterone / estradiol ratio becomes 10:1 after 6 weeks of Clomid is it a matter of concern
testosterone increased from 200 to 400 and estradiol shot upto 76 frm 22
I’m sorry, Amit, but I can’t answer personal questions about your own health. Please read the FAQ. Seeing a doctor in person would be really helpful.
Hello,
What are your thoughts on how Clomid affects Lipid panel tests (Triglycerides, hdl, ldl, total cholest.)? Is it true that clomid can cause triglycerides to rise extremely high?
Thank You
It has not been my experience that clomiphene substantially changes lipid profiles. If you are referring to yourself, you really need to see a doctor. Please read the FAQ.
Do you have any experience treating males with clomid who responded well to it in the regard that their total testosterone and LH levels increased but at the same time experienced a decrease in sex drive?
If you run into this problem do you usually start to look at their estrogen and/or SHBG levels?
Is it true that raised SHBG levels can decrease Total Testosterone?
Is it true that Clomid can raise SHBG levels?
Hi Robert, a man with such a specific set of side effects should really see a doctor. Please read the FAQ.
Correction for my above question.
I was meaning to ask if rasied SHBG levels can decrease Free Testosterone levels. (Not total testosterone)
I have been taking Clomid with Androgel somewhat consistently and have gotten great results. Your FAQ seems to imply that you really don’t know much about this combination. Is that correct? If so would it surprise you that the combination works well?
Hi Marc, I can’t answer personal questions about your own health. Please read the FAQ.
Please re-read my original question. I mention your FAQ so obviously I have read them. My question is not personal, but more wanting to know your opinion on if you would be surprised if the androgel/ clomid combination works well.
Then you read what I wrote in the FAQ, “you have no way of knowing if that is working, because you have no way of measuring testosterone inside of the testis, which is very different than testosterone inside of the bloodstream.”
Hello there! I came across your site while looking for information about how clomid works in men. 🙂
My husband and I have been trying for over a year and a half to concieve. We found out that he has low T, low count, low morphology, low motility. The docs have basically said our only option is IVF with ICSI – which wouldn’t have been a problem except my insurance (which is normally fantastic) does not cover ANY type of reproductive services such as IVF.
My husband’s urologist has put him on 1/4 of a pill of Clomid, per day, along with another pill to counter-act the estrogin rise.
My question is – from your own experience of knowing people on clomid – or anyone else out there who may know…has Clomid, in men, been shown effective in helping fertility in men who have low count/morphology?
Now, I also have a SLIGHTLY blocked tube, but otherwise am like clockwork with my cycles – no cysts, no nothing.
I’d just love to hear of any success stories of men who were able to conceive with going on clomid. thank you.
I’m sorry, Annie, but I can’t answer personal questions about your husband’s personal health. Please read the FAQ.
I was just looking for “your opinion”. You say there is no way of knowing. but….is it possible? Plausible?
My opinion is that it’s not a good idea, because you have no way of measuring testosterone inside of the testis, which is very different than testosterone inside of the bloodstream.
Thank you. My experience is purely physical in nature…I.E..I just feel better. Thank you for your opinion.!
Dear Doc,
First of all thanks for the great info.
Clomiphene blocks estrogen at the pituary. Ok, my question is, does its use have any effect on the level of actual estrogene production by the body? Can it increase estrogen production in men as it does testosterone or lower it?
My main concern is area of bodyfat deposition. I’m male but unfortunately my body deposits bodyfat mainly at the buttocks and upper legs. Can the reason for that be high estrogen levels?
I’m training with weights to get bigger at the moment and that needs a surplus of calories. Gaining muscle always goes together with gaining some bodyfat and depositing fat at more manly areas like stomach and upper body is no problem but I don’t want to put on bodyfat on my lower body.
I thought clomiphene use could help in this regard if it lowered estrogene production?
Thanks in advance
Sonny
I’m sorry, Sonny, but I can’t answer personal questions about your own health. Please read the FAQ.
Does clomiphene use have any effect on the level of actual estrogene production by the body?
Does it increase estrogen production in men as it does testosterone or lower it?
Thanks
Sonny
Coming on the heels of your last question, it’s pretty obvious that this is about your personal health. Seriously, the best way to get proper answers to your questions is to make an appointment with a doctor that specializes in male reproductive medicine and to have a conversation with him or her in person.
Hi,
I’m coming off 3+ years of continuous testosterone supplementation from my urologist.
The blood work indicates I’m not producing any LH and all the other stuff is basically shut down. The Dr. had referred me to a Endo for hormonal advise/support.
My wife and I are starting to try for a child and he felt we would be better served by an Endo. I’ve heard about Clomid for a while, along with Novadex (?), HCG, and a few other things. Thus the interest in your blog. Great quick reading, by the way.
My question is what can I expect the Endo to do, advise, test that will be taken, how long before everything might start working again?
I’m 5 weeks since my last injection, but can’t see the Endo for another 3 weeks, so I’m in the horrible rut and hoping for your advice on whether I should try to see an Endo ASAP or is there risk (in addition to the rut) that harm might be done with getting the testis going again?
Thanks
I’m sorry, Craig, but I can’t answer personal questions about your own health. Please read the FAQ.
Hello Doc,
If a ten week cycle of testosterone enanthate is used, which of the following would you recommend for pct, clomid or nolvadex?
I have no idea why a “ten week cycle” was prescribed, and it would depend on the individual patient. I would recommend that person see a physician for treatment.